Nearly one quarter of all global
internet traffic is involved in the piracy of copyrighted media, as of 2016
according to research reports by the US Bureau of Economic Analysis. That fact
by itself is shocking in scope. It’s the sort of lynchpin fact that could
easily headline a staunch anti-piracy campaign, which are more in favor now sincethe solely dramatic anti-piracy advertisements of the early 2000s were far fromsuccessful. In fact piracy bandwidth – the total data used by digital piracy –
has increased by roughly 50% annually since the premiere of the FBI’s You Wouldn’t Steal A… campaign. Growing
at an almost exponential rate, despite shutdowns of The Pirate Bay and
MegaShare, it’s clear the hydra that is 21st century piracy is not
one to die soon.
(You Wouldn't Steal A... campaign, circa 2002).
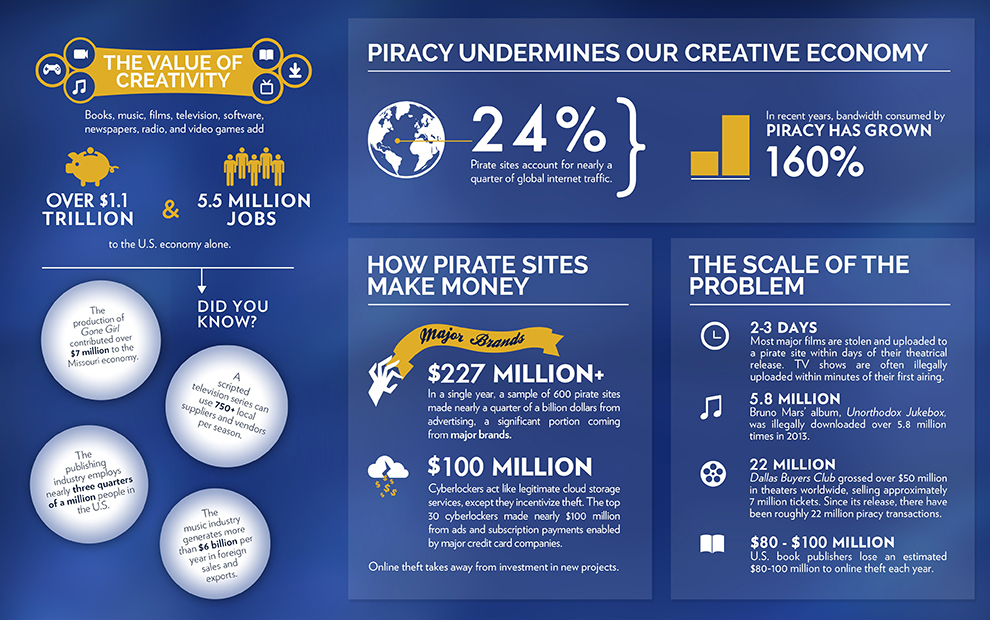
I bring up these statistics for
their precise face value, they’re numbers. Numbers evoke a very analytical and
very dry part of our brains, and just as usual as they are for objectively quantify
a situation, they are just as prone to distract. In the case of piracy, the list
of statistics are a long one, just take a look at this infographic prepared by Creative
Future – an anti-piracy group based out of Los Angeles:
Source:
Creative Future. 2016.
These numbers evoke issues that are
rooted in economics and finances, imports and exports, legal codes and
legislation. It becomes drier and drier the more we talk about it. In fact, the
US Congress has not updated the Copyright Act of 1976 since a digital amendment
was added in 1998, back when transferring a movie online would take almost a
week compared to the minutes it can be today. Congress hates debating this issue
– especially now that Google has become the single largest lobbying group in
Washington DC. Little is expected to change as our digital econoy has irrevocably
grown around our lax digital copyright laws.
There is a definite status quo with our
piracy, both legally and on a broader cultural spectrum. It is something we
have accepted worldwide as part of our 21st century lifestyle – at least
25% of the world certainly agree. And it’s a dangerous one, but not for the
numerical reasons that so cloud the issue:
Ruth Vitale (CEO, CreativeFuture) was particularly vocal
about its negative consequences. One shocking case study she noted related to
Dallas Buyers Club (for which Jared Leto won an Oscar). Jean-Marc Vallée’s 2013
film generated about 7 million theatrical ticket sales. But, it amassed some 21
million illegal downloads, or about three times more than the legal
transactions.
[Ms. Vitale later added] “It is sad whenever an artist
doesn’t get compensated for their painstaking work. In this example, though, I
do like to see an indie film like The Rendezvous and director Amin Matalqa get
as much exposure as possible.”
There’s no doubt that piracy hurts
small sleeper hits like Dallas Buyer’s
Club or The Rendezvous, and we know
that before the numbers are even presented. But there’s a cost that stretches
beyond simple box office tickets. For a film like Dallas Buyers Club, most of the crew was paid close to minimum
wage, banking on ‘back end points’ or a small percentage of the net profits if
the film did well. The film was successful, but never broke past its initial
production cost. Many of the filmmakers, as Ruth Vitale can testify, are
struggling to find work, and some may exit the film industry all together. Amin
Matalqa, after working near a decade on his feature rather apathetically admitted
it’s likely his last. And that’s the unseen cost behind the millions of tickets
we tend to focus our attention on.
We’ve all seen that seemingly more
and more superhero movies are being made each year, and hardly anything else
reaches the silver screen. That’s not simply Hollywood greed as many a
laptop-warrior might decry as he pirates The
Dark Knight for the umpteenth time, but a symptom of an industry hemorrhaging
money on smaller projects like Dallas
Buyers Club. As a consequence, less and less of these smaller movies are
being made, relying of the tentpole blockbusters to rake in the years net
profits for the studios.
Through all of this we forget that
our arts are the glue that bind us together as a society. Every year there is a
movie that fundamentally shapes the way we perceive the world. We have to look
just under a century ago to the iconic Birth
of a Nation and its distasteful blackface to glimpse into the tense racial
divisions that plagued the 20th century. Gone with the Wind brought to light Hattie McDaniel, the first
African American actress to garner the Academy Award for Best Supporting
Actress – a cultural milestone in our long history of racial injustice. And in
2014 amidst a wave of 21st century discussion of sexuality and gay
marriage, The Dallas Buyers Club
brought to light issues sexuality through the AIDS epidemic in the most
heartbreaking of stories following a homophobe stricken with HIV.
These pictorial stories aren’t just for
entertainment, but bring to light cultural issues we are waging everyday as a
global community. It’s a price that a dollar sign can’t measure, but the voices
of our creative communities cannot be stifled as we try and tackle issues of
inner city poverty, racism, and sexism. These stories carry an important weight
with a power equal if not greater than the journalists of The New York Times.
The fight against piracy isn’t a just a legal one as the FBI banner’s might
make you think, but a cultural one.
The doctor’s office is a place we
are all familiar with (that’s not to say we necessarily enjoy the visit,
especially having to reschedule our entire
Tuesday afternoon’s to hit that 3:00 PM timeslot). But outside of the slight
inconveniences of afternoon traffic or the curse of a perpetually late doctor,
our contemporary medical practices are a remarkably pain free. Once invasive
procedures can like open heart surgery can now be performed via laparoscopic
catheters – the process of inserting a microscopic camera and knife mounted a
thin plastic tube through the femoral artery1. Astoundingly the
process leaves only two quarter inch scars on the inside of the thigh a stark
contrast to the broken ribs and sternum long scar from classical open heart
surgery1. These ‘Minimally Invasive Surgeries’ as they are known are
less time intensive, have nearly half the recovery time, and most importantly
have a significantly increased survival rate relative to more invasive and
traditional methods2. Many of the bounding advances in our new age
of medicine have the digital age to thank. In the case of minimally invasive
heart surgery, the success of the laparoscopic process rests entirely on the
development of the compact and high-definition cameras used – most laparoscopes
span roughly 5 mm or half the size of your pinky fingernail2.
(Example laparoscopes, 5mm and 10 mm sizes. Source: http://www.veterinarylaparoscopy.com/userimages/laparoscopes1.JPG)
The veritable effects of these new heart
procedures can be witnessed in the turnaround of the Seattle area medical
community, which in the late 90s began embracing these emerging digital
technologies, implementing newer tools and techniques across the greater
Western Washington area3. Now thanks to the work of the Virginia
Mason Medical Group and the University of Washington Medical School the Pacific
Northwest ranks as first in the nation for heart attack, heart failure and
stroke treatment, a microcosmic testimony to the medical revolution we are
living in today3.
Sixteen short years into
the 21st century, we’ve constructed an understanding of the human
body never before conceptualized. We have the astounding capability to image, examine
and heal the body more efficiently and effectively than over more than eight
millennia of recorded medical practice. We now possess ability to detect and
decipher even the most fickle of diseases or earliest stages of cancer – thanks
to recent developments in digital imaging like positron emission technology. As
doctor and author Eric Topol notes in his novel The Creative Destruction of Medicine, the far reaching results of
digital technology have spurred overwhelming enthusiasm within the medical
community4. Topol’s sweeping interviews investigate a wide range of
opinions in virtually every specialty of medicine practiced today, and the
consensus is clearly for digital medicine4. And to mirror the novel’s
subjective social consensus, more objective scientific studies have been
assembled by the National Institute of Health investigating this very
advancement5. The findings show digital medicine having a
significant impact across medical fields in terms of patient care, quality of
treatment, and so on – proof that Seattle’s cardiology boom isn’t so much an
outlier, but a trendsetter6. Save for minor arguments relating to
the cost of more expensive digital machinery operating expenses7
(which in truth is more a political-funding issue than a medical concern), for
doctors and patients alike, there is little reason against modernizing medical
practices for a digital age.
However
there is one gross exception to this digital movement: gross anatomy.
As nearly every facet of
our medical community moves towards a digital medium, there in suit has been a
growing movement towards digitizing medical cadavers, the bodies that make up Gross Anatomy. For all the good that the
digital world brings to medicine, it is not a one-size-fits-all improvement
that extends to the paramount course that is cadaveric dissection. In fact more
damage is being done to the quality of our emerging doctors than is benefited from
the digital transition. The anatomical education every medical student receives
in gross anatomy – whether a future physician or brain surgeon – is absolutely
essential for every healthcare professional, as the body is inherently their
specialty in one capacity or another. Today in the pro-digital movement, there
is a faction of medical professionals and universities attempting to altogether
abolish the practice of cadaver dissections, favoring digital and virtual
reality teaching components instead8.
(Virtual Reality Dissections in action.)
On the surface level this anatomical
digitization a result of our trend towards our digital medical era. And while
this recent technological boom certainly has influenced the burgeoning of
digital dissection platforms and virtual reality anatomy, the fundamental shift
away from cadaver dissection stems from a much deeper cultural relationship -
and fear - of death. But in spite of the cultural taboos, the dissection of
human bodies isn’t a simply archaic tradition, but a critically formative
experience to young doctors that simply cannot be replaced by a digital model. Notwithstanding
of all the positive effects that digital medicine has on our health as a
community at large, gross anatomy is the fundamental aspect of medicine that
cannot be digitized. To
fully understand the complicated relationship we as a society have to medical
cadavers today, we must first look to the origins of human dissection itself.
In its most primordial state, the first evidence of ‘medicine’ or ‘surgery’
appears circa 7000 – 6500 BCE in trepanned skulls, the iconic craniums with
surgically bored holes9. Neolithic shamans of mankind’s earliest
societies
(A trepanned
skull, the earliest evidence of medical intervention. Source: https://upload.wikimedia.org/wikipedia/commons/thumb/5/52/Crane-trepanation-img_0507_crop.jpg/1024px-Crane-trepanation-img_0507_crop.jpg)
would drill into the skull until the white
matter of the brain was visible to the naked eye, with the belief the surgery
would release evil spirits afflicting the sick9. Today trepanning
represents the first recorded instance of health intervention by fellow man, “medicine”
in its simplest terms9. By no accounts is this rudimentary practice
a form of dissection, but it serves as a beginning on the timeline of medicine
that spans nearly nine millennia from the practice of trepanning to today. The first
seven millennia of medicine practices were exclusively dictated by religious or
tribal beliefs over any codified understanding of the human body, until
approximately two thousand years ago when Aelius Galenus - or Galen as he is
more commonly known - released his famous treatises, The Galenic Texts10. These sweeping volumes classified
the human body as never before, mapping the muscle systems, identifying major
organs and systemizing the four essential humors (black, yellow,
blood, and phlegm)10.
(A classical woodcutting describing the four humors. Source:
Though antiquated by today’s standards,
this compendium served as the primary medical text for more than fifteen
hundred years, and the basis of nearly all Western medical practices in this
time10. The classical practice of bloodletting for instance is
directly derived from the humor model proposed by Galen, believing illness to
be derived from an imbalance in the humors, thus excess blood was excised from
the infirm member’s body as remedy. And yet, despite the text’s hallowed
status, Galen never dissected a single human body – from the direct consternation
of both Christian and Jewish churches considering the desecration of any human
remains to be an excommunicable offense11. Instead Galen completed
his anatomical studies upon rhesus monkeys, relying upon their homological
similarities to the human skeleton and muscular systems. Never dissecting a
body in his time, Galen would never be aware of the inaccuracies between his
animal work and the human physiology11.
It
wasn’t until 1543, that a Renaissance doctor by the name of Andreas Vesalius
that dissection entered the modern medical practice – less than five hundred
years ago, a blink in the near nine thousand years of medical practice.
Vesalius, an established professor and surgeon of Padua began a series of
lectures of live dissections for his disciples, performed on the bodies of
deceased criminals, deemed by the church to be beyond reproach and fit for
post-mortem examination12. His findings were shocking, and often
contradictory to the Galenic teachings that were so prominently disseminated at
the time11. For instance, Galenic text asserted that all blood
vessels originated in the liver, as opposed to the heart11. Vesalius
would compile his work into his magnum opus, De Humani Corporis Fabrica Libri Septem12. Over years of
work in dissection, Vesalius and his pupils would compile one of the most
extensive anatomical charts of the human body, each system expertly illustrated
in his seven part book.
(An Andreas Vesalius
illustration. Source: https://nyamcenterforhistory.files.wordpress.com/2014/10/vesalius_fabrica_1543_lambert_181_watermark.jpg)
The combination of precision in and
fundamental reconstruction of the Galenic model, Vesalius’ work opened the
doors for truly modern medical practices. With an accurate anatomy of the human
body, the antiquated Galenic models were discarded and modern surgical
practices quickly evolved under the newfound anatomical understanding11.
Surgeons could avoid arteries during amputations, and gallstones could be more
easily pinpointed, the influence of an accurate anatomical topography was endless11.
Mixed with the fancy of the Roman Emperor Charles V, and the advent of the
printing press, Vesalius’ work would travel like wildfire across Europe in even
into Asia and North Africa12.
Despite the widespread popularity of De Humani Corporis, acceptance of
dissection did not spread with the manuscript. In fact as the documents
travelled across country borders, laws were enacted against the sourcing of
human bodies for dissection. Several decades after the first publication,
turnover within the Catholic Church led to more punitive measures against
surgeons dissecting human remains for medical purposes than under the previous
pope12. And so as medicine advanced, developing doctors began
illegally “body snatching” in order to practice anatomy and surgical techniques
on a human specimen11. Without a legal means in nearly every
country, the banned practice remained in place consistently through the 20th
century. In the United States in particular, body snatching was common practice
through the 1960s, until the Anatomical Donation Act was passed allowing for
citizens to preemptively sign away their bodies to science13. Though
no concrete statistics exist to quantify the extent of the illicit practice,
the demand bodies across several thousand medical schools relative to the
meager legal channels (dead federal prisoners) suggests a large percentage if
not came from graves up to fifty years ago11.
Now after half a century
of legal cadaver dissection we’ve begun to reverse the process of nearly nine
thousand years in the making. Spearheaded by some of the United States’ top
medical schools, there is a significant movement to altogether end the use of cadavers
from the medical school curriculum. In 2011, Stanford University made wakes
within the medical community introducing their ‘virtual dissection table,’ a
backlight surgery table that illuminates human cross sections, and at a fingers
touch can dissolve from cross section to cross section, progressing through the
body14. An eminent figurehead of the medical school community, other
schools in the San Francisco Bay area followed suit introducing similar virtual
dissection tables to supplant a traditional cadaver lab15. A year
later, St. Mary’s Hospital in London proudly became the first major European
Hospital to incorporate virtual technology into their curriculum16. In
a few short years, Stanford has halted all use of medical cadavers on its
campus. And the epidemic is spreading quickly across the US and abroad as these
once $300,000 tables are becoming more and more economical for smaller
universities to afford15.
It is clear we are now in
a transitory period in our use of cadaver labs, and it begs the question, “Are
virtual dissections better?” While there are accessory interests, and financial
incentives in moving towards a virtual lab, the absolutely essential product in
question in the quality of doctor produced. That is a quality that no price tag
can measure up to. And by this metric alone, the virtual dissection fails. Seldom
does the word “never” appear in scientific literature, there is an inherent
danger with speaking in absolutes. Yet in 2008 the ASME concluded this, “We
recognize that virtual dissection will never
provide the same hands-on experiences as physical dissection”17. And
that is the core fault of virtual dissection exposed by an objective study. A
physical, hands-on experience cannot be supplanted by clear cut virtual slides.
“There is form of somatosensory learning that cannot be formed without
physically engaging in the activity.”17. This fundamentally
undermines perhaps the most important facet of a doctor’s education, their
physical abilities, in a profession that is so inherently tactile. This isn’t
to say that virtual reality models are not in some way useful. A recent study
has shown that virtual reality models helps increase the ability for gastroenterologists
to detect colon polyps at a significantly higher success rate than doctors
operating without virtual reality training18. The distinction is this
study uses virtual reality as a secondary method to augment medical practice
over supplanting physical activity altogether17. Virtual dissections
can make for an extremely useful tool to augment the learning of our young
medical students, and even as a practice space for our most seasoned doctors,
it simply cannot be used in place of the real body.
But the true impact of a
course like gross anatomy is less so a matter of book education of dexterity,
but as forge to temper the emotional maturity of our up and coming medical
professionals. For forty-three years Dr. Snow, Ph.D has led the new medical
students of USC Keck through their first human dissection, a process that
begins with the back and slowly – over the course of a year – moves eventually
to the face. He explains it’s a process adjusting to death, not in the way of
accepting a grandparent’s passing, but accepting the death of a complete
stranger – a sad but constant part of a job as a doctor15. And for
the first class, the students simply acclimate to the chilled body locker. And
while the image of forty or so bodies draped in sheets in a ghastly one to
most, the student transformation by the end of the term is anything but. In the
process of working with the bodies, which is on a near daily basis the students
become incredibly close over the months they spend together15. They often
name the cadavers (though they are never given their actual names for confidentiality),
affectionately giving a personality to the man or woman that so generously donated
their body for their benefit. Second year USC medical student Natalie Hartman
best summarized her experience with her donor affectionately named ‘Admiral
Victor,’ as such, “He was our first real patient. He was the first person to
trust you with all of the insecurities and ailments of his body. And that’s a
special connection.”19 In an industry founded upon doctor-patient
relationships, this is an irreplaceable form of learning and maturation that
cannot be forced or coerced on a virtual reality holodeck.
So why are we still moving away from medical
cadavers? In reality, the motive less a scientific one, but an emotional one
more than nine thousand years in the making. The same cultural forces that
opposed dissection during the time of Galen, and after the rise of Vesalius
still echo today. Across regional and temporal lines, the resistance to medical
dissection is distilled into a in a common theme: our relationship with death.
There is something sacrosanct in the deceased that we all share, with no definite
answers, nor explanation of what happens after death, we revere it, and we fear
that which cannot fathom. Emotions and fervor trumped scientific and medical
reason - it became easier to avoid the controversy by outlawing the practice
than by permitting. Even today with the complete legality of medical cadaver
sourcing, it still is a somewhat controversial topic, because of the uneasy
nature of the subject, and that is something that simply is ingrained into our
cultural perception of death. Other accessory arguments can be made toward the money
spent sources bodies, and the difficulty there is in the process of acquiring
donors. Likewise similar arguments can be made towards the whole digital
movement of the medical industry as a whole. But as previously stated, the product
is not measured in the dollars saved, but the quality of the doctor, and we
cannot afford to short change our future doctors by taking the easy way out. Medical
dissection like the Hippocratic Oath are not tradition within medical practice without
good reason. They have been preserved over hundreds and thousands of years for
their fundamental role in foundationally shaping the quality, expertise and
above all caring that our doctors are expected to exemplify. It is just as much
emotional as it is an intellectual commitment, and one experience we cannot let
subside to the digital wake.
The final stanza of poem written by Warren
Yamashita in memory of his cadaver perhaps best summarizes the lasting significance
gross anatomy has on its subject:
“I promise, you
are the first and last human being I will ever dehumanize.
I’m sorry for
stabbing your heart, thank you for convicting mine.”20
An editorial note from the writer:
I choose to begin not at
medical cadavers, but with a note about heart surgery in the Seattle area. This
wasn’t to hide my thesis pages deep into this article, but to provide some all
too important context on the relationship of the digital world to medicine in
this complicated issue. Had it not been for a surprise diagnosis in my junior
year of high school, I might not be as aware as I am today. In 2011 I was diagnosed
with a congenital heart defect that required surgery. In the terrifying process
of preparing for heart surgery I was able to witness the effect that these new
technological leaps in cardiology – and leap is an understatement – that have
been made in the last several years. The surgery I opted, a minimally invasive
catheter ablation for had a 92% survival rate at the Seattle Children’s
hospital. Had surgery become necessary two or three years earlier, before the
necessary laparoscopic camera had been developed, the open heart conditions
would have dropped by survival rate to about the flip of a coin.
With an issue like medical
cadavers that is a complicated nexus of so many conflicting perspectives, it’s
an issue that can quickly become obfuscated with one voice or one viewpoint too
strongly represented. Within this argument there is a very serious case to be
made towards the preservation of cadaveric dissections, and non-digital methods,
especially in consideration of the quality of the doctors we are producing. In
many respects this is an issue much less about survival rates, but on the
cultural relationship we have with death, and for good reason we as a culture
are weary of cutting up our fellow man. This traditionalist view of medical
cadavers that I want to avoid from blinding the larger issue at play: that is
the ever increasing relationship of medicine and digital technology. For all
the ardent support I will put towards the continuation of medical dissection, I
cannot ignore the profound and important impact emerging digital technologies, for
me, my very life, my family, my hometown of Seattle, and the global community
at large.
In a world with so many
changing parts, from changing presidencies to changing gas prices, we have a habit
of comparing then to now; past to present. While we’ve made so many fundamental strides within medicine, we
can’t ignore what has worked in the past to favor a new trend the present,
simply because of a false dichotomy we’ve created between old and new. New has its
place, be it catheter heart surgery or PET scans, but cadaver dissection has
persisted through centuries of hardship and illegality, and not without good
reason. Young doctors need the experience; it’s something indelible that simply
cannot be faked. Gross anatomy is just as much a part of the Renaissance age of
Vesalius as it is now at the USC Keck School of Medicine, Fall Semester
2016.
End
Notes:
1Minimally
Invasive Heart Surgery. (2016). Mayo
Clinic. May Clinic Tests and Procedures. Retrieved
from: heart medicine: http://www.mayoclinic.org/tests-procedures/minimally- invasive-heart-surgery/basics/definition/prc-20013701
2Minimally
Invasive Heart Surgery. (2009). Brown University.
Department of Biomedical Sciences. Retrieved
from: http://biomed.brown.edu/Courses/BI108/BI108_2000_Groups/Heart_Surgery/
3Komo
News: Seattle. Seattle Hospital Ranks
Among Best for Heart Surgeries. Retrieved from:
4Topol,
K. (2012). The Creative Destruction of
Medicine: How the Digital Revolution will Create
Better Health Care. New York: Knopf. Retrieved from: https://books.google.com/books?hl=en&lr=&id=I6Bgje2T7Q8C&oi=fnd&pg=PT5&dq= digital+medicine&ots=ipXFUf8giY&sig=9adCD74kWSulgrnUFB5xHeswuOk#v=onepa ge&q=digital%20medicine&f=false
5Shaffer,
D. (2002). What is Digital Medicine?
Stud Health Technol Inform. 2002; 80; 195-204. Retrieved
from: https://www.ncbi.nlm.nih.gov/pubmed/12026129
6Elenko,
E. (2015). Defining Digital Medicine.
Nature Biotechnology. 33, 456–461 (2015) doi:10.1038/nbt.3222.
Retrieved from http://www.nature.com/nbt/journal/v33/n5/nbt.3222/metrics/index.html
7Terhune,
C. (2009). The Dubious Promise of Digital Medicine. Business Week. April 2009. Retrieved from: http://securehealth.freshdefense.net/content/dubious.pdf
8Reidenberg,
J. (2002). The new face of gross anatomy. The Anatomical Record. doi/10.1002/ar.10076/full
13University
of Arkansas. (2010). Gross Anatomy: Then
and Now. College of Medicine History. Retrieved
from: http://medicine.uams.edu/about-the-college/college-of-medicine-history/history- features/gross- anatomy-then-and-now/
14Stanford
University. (2011). Body image:
Computerized table lets students do virtual dissection. Stanford Medicine. Retrieved from: https://med.stanford.edu/news/all-news/2011/05/body-image- computerized-table-lets-students-do-virtual-dissection.html
15M.
Snow. Interview. September 5th, 2015.
16BBC.
(2012). Virtual surgery: How to dissect a digital cadaver. Retrieved from: http://www.bbc.com/news/technology-18173263
17McKenna,
A. (2008). The American Society of Mechanical
Engineers. Paper No. DETC2008-49783, pp. 359-368;
10 pages doi:10.1115/DETC2008-49783
18Hock, D. (2007). Virtual
Dissection CT Colonography: Evaluation of Learning Curves and Reading Times with and without
Computer-aided Detection. RSNA Radiology. DOI: http://dx.doi.org/10.1148/radiol.2482070895.
Retrieved from: http://pubs.rsna.org/doi/abs/10.1148/radiol.2482070895
19N.
Hartman. Interview. September 4th, 2015.
20 W. Yamashita. Personal
Correspondence. September 11th, 2015.
In the
final weeks of this bloated election season we are catapulting towards a Nov 8th
election night that is surely going to alienate a significant portion of the American
population by the outcome - and not that previous elections haven’t
precipitated in fierce politicking across the aisle. Take for instance Mitch
McConnell’s remarks to, “Make Obama a one term president,” following
the 2008 election against McCain. But this election is different. In truth it’s
not so much an election as it is a war. To voters across the political
spectrum, the candidates aren’t the opposition, they are the devil incarnate. There
has been so much animosity drudged up by this election it begs the question,
will we as a country be remotely satisfied if either Trump or Hillary are
elected to office?
The
short answer? No. An Op-Ed in The Atlantic took note of the post-election
fallout for Trump supporters – assuming a likely Hillary victory:
It leaves Americans that
much more segregated and alienated from one another. It’s exactly this kind of
cross-cultural suspicion and mistrust that has enabled Trump to come within
spitting distance of the presidency. And it’s what threatens to keep his supporters
isolated and fuming on the sidelines, long after their champion has forgotten
them.
But it goes further. Much further. Trump’s
incendiary remarks have not only lit a fire under his most ardent supporters,
but scorched a thick division between the Trump right and the center that not
even members of his own party can transgress. If even a quarter of Trump’s ludicrous plans
come to fruition, not even his own party can potentially stop it. Even the RNC establishment has
blacklisted Trump – pulling funds to the RNC Victory Campaign, one of the
largest sources of campaign money to Republican campaigns. In a terrifying way,
Trump has aggravated a significant faction of the US population by alienating
them from the rest of the country. It’s Us
versus Them. “The liberal media says…They wanted that story to drop…I’m not
perfect why are they…” Through this mentality Trump has convinced 40-45% of the
country to buy only one brand, Trump.
And if they lose, where will they go, and will they be satisfied? I doubt it.
Trump
is a sore loser, despite his outrageous debate comments towards his, “winning temperament.”
Undoubtedly Trump’s post-election media presence will be massive, and all the
more inflated by his seemingly inevitable lose. But the damage has already been
done, he has become the de facto (and only voice) of such a staggering
percentage of the American public, that he can continue to drive this political
division long after the election. If you don’t believe me, just look at how
effective his Twitter has been in his campaign. Like him or hate him, Trump is a
master of social media. The rumblings of a Breitbart-Trump news channel would take this twitter-talk to a national level post-election.
But the
point I’m making isn’t just about Trump. In the unlikely, but ever so possible
chance that Trump loses the election, we are back to the same alienated place
that pending a Hillary victory. The sad fact of the truth
is that the scorched division between the Hillary camp and the Trump camp goes
two ways. Should Trump win, undoubtedly it would be rejected by democrats and
moderates across the country. Riots, hate speech, you name it. Our attention would be the Sanders, Clinton and
any other liberal voice to speak against president Trump. And without a doubt
every month of a Trump presidency would be a fight against the liberal
establishment. But the bottom line is this action will be just as politically toxic as a Trump victory.
As we
move forward from this pivotal election, we as a country need to realize that
the wounds we have inflicted across the aisle are not ones that we be magically
healed as of November 9th. These are long lasting issues that will
alienate half of our country in a way we haven’t seen before. And there isn’t a
one size fits all solution to this malady, but it is a problem that cannot be
ignored as we go into the 44th President of the United States’ new
term.
2016 has been loaded with
sequels. Finding Dory, The Purge 3,
Neighbors 2: Sorority Rising, the list goes on and on. And sure the three
aforementioned titles grossed millions of dollars domestically this summer, but
there’s a different sequel you haven’t heard about racking in just as much
serious coinage over this summer. (SPOILER ALERT: It’s not a film).
Much less scintillating than a
Hollywood Earthquake flick, the recent ruling of McCutcheon v. Federal Election Commission has done just as much to
shake up the 2016 election. Essentially the decision has cast away the cap on
individual contributions to political campaigns installed during the 70s under
the Federal Election Campaign Act of 1972. The New York Times further details the slackened legislation:
After the McCutcheon decision, Mrs. Clinton
established an agreement last year with the Democratic Party under which she
asked her wealthiest patrons to write checks in excess of $300,000, more than
double the old limit.
Because there are no limits on how much
money party committees can transfer to one another, most of the state parties
have cycled their share back to the Democratic National Committee. The party
then moved the cash into a smaller number of battleground states to prepare for
Election Day.
Ironically the decision has been
decried by much of the Republican establishment that was once proudly touting
the Citizen’s United v. Federal Election
Commission decision as a landmark in the reformulation of our nation’s
campaign finance policy – the very decision that declared “money the equivalent
of speech” and spurred the burgeoning of the super-PAC era of American politics.
(Source:
Sunlight Foundation, 2016)
The most notable impact so far
is opposite of the original Citizen’s
United proponents intentions. The conservative think tank organization’s
lobbying has resulting in more than $100 million dollars donated to the Clintoncampaign over the Trump campaign. Democrats have taken advantage of the recent
ruling to increase campaign funds by uncapped personal donations to the Hillary
Campaign fund.
This development in the arc of American
campaign finance isn’t about the schadenfreude liberals can gloat in, but the
frightening revelation in our nation’s politics that the original liberal
antagonists of the Citizen’s United
case are now fully embracing the second coming of the landmark decision with McCutcheon. (And while Hillary voiced dissent
to the 2014 decision, her full force embrace of the decision in her campaign
finance tells a different story).
And perhaps the Democrats aren’t
completely to blame for exercising their right to fundraise (especially during
such a toxic and pivotal election). But it does pose a dangerous look at our
runaway campaign finance policy, especially when the original opponents are now
embracing the decision at a $100 million advantage. Does this mean that soon
our elections can truly be bought by handful of the wealthy? Once upon a time,
that was hyperbole thrown around in New York Times Op-Ed’s, but now that might
be a real possibility in the next few elections.
To take it back to Hollywood analogies,
sequels rarely do live up to their originals (Jaws 2 anybody?). But this is a
sequel we need to be talking about,
yet nobody is.